To improve cancer and chronic disease prevention and screening for cardiovascular disease, diabetes, osteoporosis, and colorectal, breast, cervical, prostate and lung cancers and their associated risk factors in patients 40-69 years of age.
Areas of Focus
Training of BETTER Prevention Practitioners™: provide hands-on training of healthcare professionals on the Prevention Practitioner role and BETTER approach.
Continuing Education: provide learning opportunites for inter-professional healthcare providers and learners to help implement prevention and screening guidance and inform patient care.
Implementation Support: provide tailored implementation and adaptation support to primary care practices and organizations interested in adopting the BETTER approach.
The BETTER Institute was originally funded by the Canadian Partnership Against Cancer (CPAC) as a three-year pan-Canadian initiative from April 2018 – March 2021 as the BETTER Prevention Practitioner Training Institute. The aim of the initiative was to support the long-term uptake and sustainability of the BETTER approach to cancer and chronic disease prevention and screening in primary care settings across Canada.
One of the main priorities of the BETTER Prevention Practitioner Training Institute was to work with rural, remote, and Indigenous communities to help address their healthcare needs, with a specific focus on prevention and screening.
In 2020, this initiative evolved into a not-for-profit organization – The BETTER Institute – which was dissolved in 2025. The graphic below illustrates the successes achieved from 2018 to 2025.
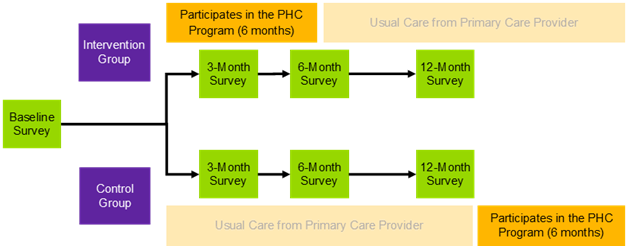
The BETTER Program has been successful in helping women initiate healthy lifestyle behaviours to prevent adverse health outcomes. However, it is not feasible to fund Prevention Practitioners to offer repeated follow-up encounters over the period of time needed to turn initial lifestyle behaviour changes into long-term habits. There is growing awareness that lay health coaches can improve and extend the quality and value of primary care. The BETTER Women pilot program is an extension of the BETTER Program, pairing women aged 40-65 with peer health coaches after their initial Prevention Visit. Peer Health Coaches (PHCs) are trained volunteers, who support women over a six-month period to achieve and maintain their health goals.
The pilot program will run for approximately three years (June 2021- August 2024) and is funded by the Public Health Agency of Canada, Canadian Cancer Society and Women’s College Hospital Foundation. The primary objective is to assess whether adding the six-month peer health coaching intervention to the BETTER Program, for women aged 40-65, leads to a greater achievement of evidence-based targets for chronic disease prevention such as decreased smoking, increased activity as well as cancer screening.
The BETTER Women Program will comprise the following stages:
Design.A PHC Training Program was developed by experts and a team at the Canadian Cancer Society, with input from research team members with expertise in similar programs. The program was competency-based and designed to prepare volunteers to be PHCs with the knowledge, skills, and confidence necessary to use motivational interviewing techniques and brief action planning to support behaviour change. The Canadian Cancer Society is currently facilitating the recruitment and training of volunteers to become PHCs. To be eligible, volunteers must be a woman between the ages of 40-65 years; have experience achieving at least one of the evidence-based behaviours under evaluation, comfortable using computers and the Internet; able to attend PHC training sessions and commit to volunteering three to four hours a week; and able to read, write and speak English. Volunteers for the Summerville Family Health Team site will also be required to self-identify as South Asian and able to speak English. A subset of volunteers will also be able to speak other South Asian languages that are common within the Summerville Family Health Team, such as Punjabi, Hindi, or Urdu. Volunteers meeting screening and eligibility criteria will participate in the custom designed PHC training program before being matched to a patient to provide coaching.
Implementation. BETTER Women will be implemented at three primary care clinics in Ontario: Women’s College Academic Family Health Team (a large urban academic, hospital-based clinic), Summerville Family Health Team (a suburban clinic where the intervention will focus on the South Asian population), and Barrie and Community Family Health Team – Family Medicine Teaching Unit (a large clinic with a greater proportion of patients from rural areas).Women aged 40-65 will be invited to participate in the BETTER Women pilot program during their Prevention Visit with a Prevention Practitioner. Interested women will be sent information on the program via mail and email. If a woman decides to participate, she will complete a baseline survey with questions about her health and health behaviours. Once completed, she will be randomized to one of two groups: the intervention group or the wait-list control group. More information about recruitment and eligibility can be found on https://clinicaltrials.gov/ct2/show/NCT04746859. Participants in the control group will be matched to a PHC 12 months post-enrollment. Participants in the intervention group will be matched to a PHC right away. Once matched to a peer health coach, participants will have weekly coaching sessions with their peer health coach in months one to three, and monthly coaching sessions in months four to six. Coaching sessions can occur through a variety of methods including phone, email, video calls, or text messaging. Frequency of coaching sessions may vary based on participant needs.
Evaluation. Several aspects of the program will be evaluated, including the PHC training, program effectiveness and implementation. Evaluation of the PHC training program will include pre- and post-training surveys, as well as focus groups with PHCs to assess the feasibility, acceptability, and effectiveness of the training in preparing PHCs for their role. Program effectiveness and implementation will be evaluated through the BETTER Women trial: a three-site, pragmatic, wait-list controlled, randomized, Type 1 hybrid effectiveness-implementation trial with blinded outcome collection after 12 months. Outcome data will be collected via surveys and chart reviews. The success of the program will be assessed by comparing the number of women in each group who, from baseline to 12-month follow-up, increase the number of targeted actions completed for chronic disease prevention and cancer screening. The multi-method, embedded process evaluation will examine the program’s sustainability, acceptability, cost effectiveness, and other factors that might affect future spread and scale. Data sources for implementation outcomes will include program data, participant surveys, and qualitative interviews with participants, prevention practitioners and PHCs.
Emerging evidence from the BETTER HEALTH: Durham study supports the need for exploration of adaptation of the BETTER HEALTH intervention for younger adults living with low income. People with lower income are more likely to be smoking, physically inactive, and lacking in fruit and vegetable consumption than those with higher income and thus are more likely to develop multiple chronic conditions earlier.
The goal of the BETTER Life study is to learn if the BETTER HEALTH: Durham program, which has been shown to help people 40-64 years take steps to prevent chronic disease, can be adapted for younger persons ages 18 to 39 years. We will focus on selected priority health neighbourhoods in the Durham Region of Ontario (identified by the Durham Region Health Department and community partners) and request feedback from eligible community residents. We will also ask community residents to participate in adapted prevention practitioner visits to determine whether sessions are acceptable to them as a means of addressing chronic disease prevention and screening needs. The study builds on existing infrastructure of the BETTER program, the BETTER HEALTH: Durham research team, community advisory committee, and primary care group from the BETTER HEALTH: Durham study.
Specific study Objectives:
The BETTER Life study will:
seek to understand individual, interpersonal and structural-level barriers to chronic disease prevention for younger adults living with low income using qualitative interviews and focus groups;
adapt the BETTER HEALTH intervention based on these interviews and focus groups with younger adults as well as key stakeholders in multiple provinces (Ontario, Alberta, Newfoundland & Labrador;
conduct acceptability testing of the adapted intervention with a small number of younger adults with low income in preparation for a future randomized trial.
Considerations
Current restrictions from the COVID-19 pandemic may not allow for in-person recruitment strategies, data collection or prevention practitioner visits. The BETTER Life research team will follow all Public Health guidelines for the Covid-19 pandemic and/or hold meetings virtually if in-person gatherings are not allowed.
Funding and timeline
This research is supported by a Canadian Institutes for Health Research (CIHR) catalyst grant and will be implemented between March 2020 and March 2022.
The BETTER Life is a study led by researchers at Women’s College Hospital, the University of Toronto, Sunnybrook Health Sciences Centre, St. Michael’s Hospital, University of Alberta, Memorial University, and Durham Region Health Department.
Learnings
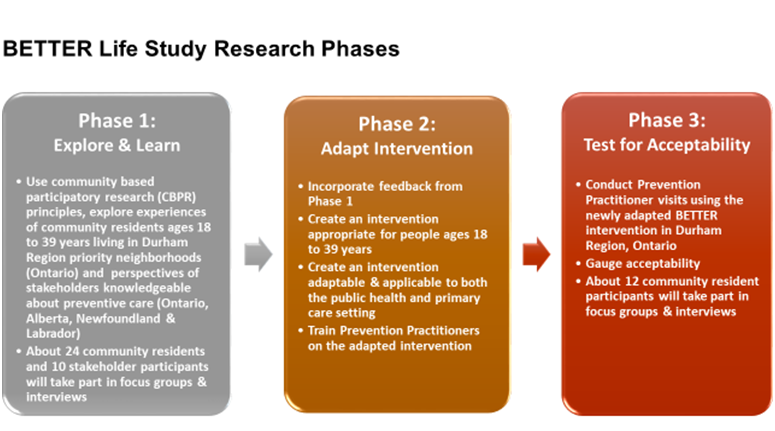
The BETTER Life study’s timelines were shifted to accommodate emerging healthcare priorities during the COVID19 pandemic. As a result, the study’s research phases were completed between October 2021 and November 2023:
Phase 1 – Explore and learn: October 2021 to November 2022
Phase 2 – Adapt intervention: April 2022 to March 2023
Phase 3 – Test for acceptability: April 2023 to November 2023
The BETTER program has shown the efficacy of using personally tailored one-on-one, in-person prevention visits to increase patients’ chronic disease prevention and screening practices. Given the recent events of the COVID-19 pandemic, however, the use of virtually-delivered healthcare services has been on the rise. While essential in ensuring that some services can still be delivered to patients, little is known about how virtual delivery affects patients’ health outcomes and how populations with limited access to technology, in particular, are impacted.
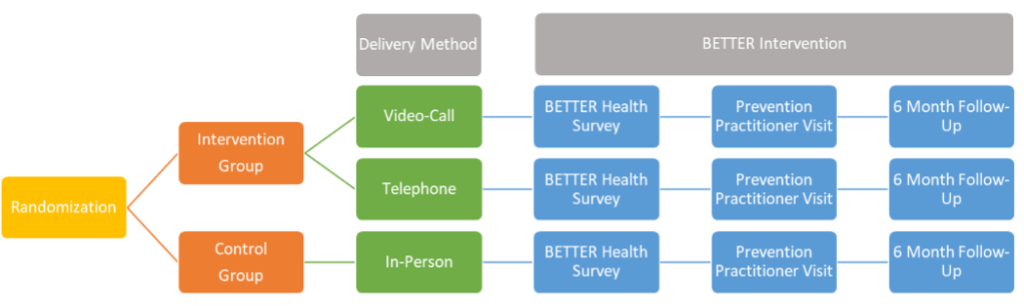
The Virtual BETTER study, which will be based out of Newfoundland and Labrador, will test the BETTER approach delivered via video-call, telephone, or in-person. We will compare things like how many patients agree to participate in a prevention visit by video-call, by telephone, or in-person, whether they were able to connect for the visit successfully, and how they rated their satisfaction with the visit and the quality of the communication with the provider. This information will be used to inform current plans to deliver BETTER and other programs using video and phone. We will also use it to plan for a larger and longer study to compare patients’ behaviour change and uptake of disease screening tests when these different communication methods are used. The results of this study will help shift the focus of the health system towards disease prevention rather than treatment and will help increase accessibility to healthcare.
The Virtual BETTER study will ask the following questions:
Do patients report similar readiness to implement lifestyle changes after video-call, telephone, and in-person BETTER Prevention visits? Are there factors such as sex, gender, age, or socio-economic status that affect this association?Are there differences between accessibility and acceptability of the different types of visit?
Are there differences between accessibility and acceptability of the different types of visit?
Are there differences in satisfaction and the rating of communication issues between patients randomized to the different visit types? Are there factors that affect this association?
Are the proposed recruitment, randomization, and data collection methods feasible and sufficient to complete a larger trial within the constraints of available funding opportunities?
Although most patients have multiple risks, most guidelines and resources are focused on one specific disease, organ system, or lifestyle risk. Furthermore, cancer survivors and patients living in poverty achieve fewer prevention and screening goals and patients may lack awareness of how lifestyle contributes to cancer and chronic disease. Building on the work of the BETTER trial and the BETTER 2 program, the BETTER WISE (Building on Existing Tools to Improve Cancer and Chronic Disease Prevention and Screening for Wellness of Cancer Survivors and Patients) project will conduct an intervention that includes electronic tools, pathways for cancer survivors, and a tool that screens for poverty.
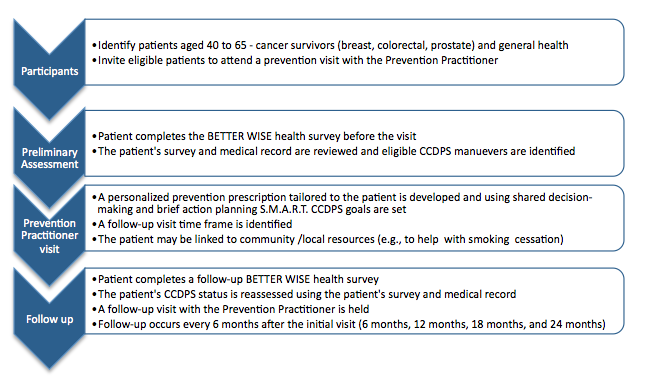
BETTER WISE is a 6-year project (2016-2022) that brings together diverse stakeholders (policy, practice, research, patients) in Alberta, Ontario, and Newfoundland and Labrador. The primary objective of the BETTER WISE project is to determine if patients aged 40-65, including cancer survivors (breast, colorectal, or prostate) and general health patients (i.e., patients without a previous history of breast, colorectal, or prostate cancer), randomized to receive an individualized visit with a Prevention Practitioner have improved cancer surveillance and general prevention and screening outcomes determined by a composite index as compared to standard care in a wait-list control group twelve months after the initial prevention visit
The BETTER WISE project will comprise of 3 phases:
Knowledge harmonization and integration – Working with primary care practices and Prevention Practitioners, a revised BETTER WISE tool kit will include blended care pathways for cancer survivors (breast, colorectal, prostate) and cancer and chronic disease prevention and screening (CCDPS), including behavioural lifestyle risk factors and a screen for poverty.
A pragmatic cluster randomized controlled trial – Sixteen primary care practices, 8 in Alberta, 4 in Ontario, and 4 in Newfoundland and Labrador will participate in the project. It is expected that 2-10 primary care providers (PCPs) from each primary care practice will be engaged, for a total of 64 PCPs across the 3 participating provinces. Patients will be randomized at the physician level to receive an early BETTER WISE intervention or to wait-list control. The BETTER WISE intervention is depicted below.
Evaluation of the impact of the intervention – The main outcome for the project will be the individual patient-level summary composite index defined as the proportion of CCDPS maneuvers for which the patient was eligible at baseline, that is met (according to pre-defined targets) at 12-month follow-up. Qualitative methods will be used to explore the facilitators and barriers to the implementation and uptake of the BETTER WISE intervention as well as to address any modifications needed to scale and spread the approach and the PP role. An economic assessment will also be undertaken to inform the health care payer and policy makers of the projected cost-benefit impact of investing in the BETTER WISE approach.
For more information about the BETTER WISE project, please contact us.
More information on the Prevention Practitioner role can be found here.
Published results from the BETTER trial can be found here:
The BETTER WISE project is made possible through a financial contribution from Alberta Innovates – Health Solutions.
The BETTER WISE Project Team (2016 – 2022)
Project Lead:Dr. Donna Manca Project Co-Leads: Dr. Kris Aubrey-Bassler, Dr. Denise Campbell-Scherer, Dr. Eva Grunfeld, Dr. Aisha Lofters, Dr. Melissa Shea-Budgell Collaborators: A. Bencivenga, G. Bloch, J. Britten, J. Carroll, C. Davis, E. Denga, K. Dong, R. Elford, L. Green, N. Hans, F. Janke, D. Klein, P. Krueger, C. Leduc, R. Lewanczuk, K. McBrien, C. Meaney, R. Moineddin, C. Nykiforuk, M.A. O’Brien, S. Oddie, A. Pinto, M. Rose, S. Ross, G. Salvalaggio, C. Scrimshaw, N. Sopcak, W. Tink, M. Wilson Community and Policy Partners: C. Campbell, C. Chan, P. Corcoran-Mooney, A. Gogan, R. Hiscock, J. MacWhirter, F. McCrate, B. Meade, K. Milley, R. Goodyear, A. Robinson Vollman, T. Wong Statistical Analysis: R. Moineddin, C. Meaney. Economic Assessment: K. McBrien Project Coordination: C. Fernandes, M. Chow, I. Khalil, K. Sivayoganathan Research Assistant: D. Ofosu Students/Trainees: M.K. Blackbyrne, I. Carneiro, M. Kebbe, C. McCartan, F. Nagase, D. Patel, S. Yildirim-Erbasli
The BETTER HEALTH: Durham study, jointly funded by CIHR and the Canadian Cancer Society, is a study that extends the BETTER Program approach. It consists of a supportive meeting to review chronic disease prevention and screening (CDPS) between a public health nurse taking on the role of Prevention Practitioner and a participant between 40 – 64 years of age who resides in Durham Region of Ontario.
BETTER HEALTH: Durham brings together investigators from Sunnybrook Health Science Centre, St. Michael’s Hospital, Durham Region Health Department and University of Toronto Family & Community Medicine. This project will span from 2017 to 2020.
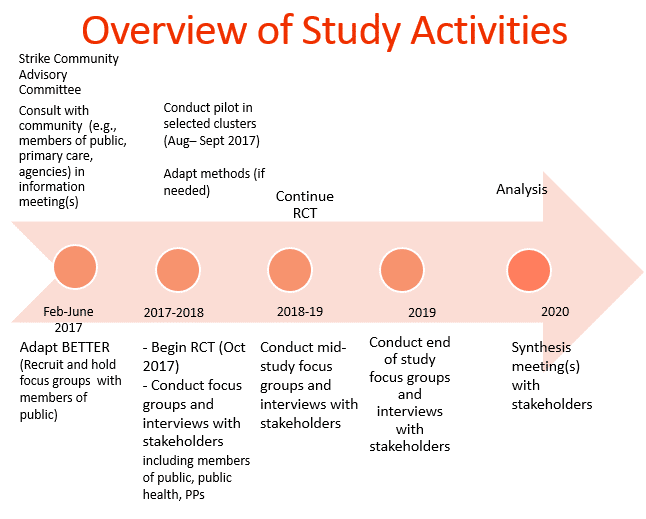
Our goal with BETTER HEALTH: Durham is to adapt the BETTER intervention guided by community-based participatory research (CBPR) principles. Participants are eligible to participate based on the ‘clusters’ where they reside. Clusters are smaller neighborhoods identified as ‘priority neighbourhoods’ by Durham Health Department, and neighbourhoods where cancer screening uptake is known to be low.
Our first phase was the adaptation phase that spanned February to July of 2017. This included conducting focus groups and one-on-one interviews with members of the public and key informants to review preliminary changes of tools, resources and setting. The linked report reviews 5 themes which resulted from this phase.
The second phase, cluster randomization, will aim to have 5 intervention (immediate) and 5 control (wait-list) clusters with 12 participants in each cluster for a total of 120 participants. The intervention arm participants complete a baseline survey by the research coordinator, complete the prevention practitioner visit and then complete their follow up survey 6 months after. For control participants, they are scheduled for their baseline survey, complete their follow up survey in 6 months and then meet with the prevention practitioner. During the visit with the prevention practitioner, the participants are able to set goals, see where their health is at and be connected to other agencies and resources through the Public Health Nurses’ extensive knowledge of community. Participants have been recruited through many means. Some examples of recruitment strategies include: attending local events, newspaper ads, posting recruitment flyers at various approved agencies and communities, Canada Post mail-out, presentations at agencies, social media etc.
The third phase, a qualitative evaluation will take place with enrolled participants, stakeholders and partners throughout the study, who will be asked to answer a range of questions from their experiences to their thoughts of implementations of the study. The qualitative phase will be based on grounded theory principles and informed by the Consolidated Framework for Implementation Research (CFIR).
Through these phases, we plan to share the adapted BETTER knowledge with a wide range of stakeholders, including policy makers, advisors, public health, primary care, community and national organizations, and with the larger research audience, using the Knowledge Transition (KT) plan.
Below compares the original BETTER study in primary care to BETTER HEALTH: Durham.
BETTER in primary care practices
BETTER HEALTH: DURHAM
Physical location of prevention practitioner (PP)
In primary care team clinics
Embedded in Health Department, Durham Region, for community outreach
Identification of participants
From electronic medical record
Community-based recruitment strategies
Identification of completed and current behaviours and activities
From electronic medical record, and from self-report in self-administered survey
From self-report responses to survey administered by research coordinator
Identification of risk factors
Lab tests, survey, electronic medical record
Self report
Motivational interview by PP and goal-setting by participants
By prevention practitioner in primary care team clinics
By prevention practitioners at various community locations
Facilitation of goal achievement
Clinic staff, prevention practitioner, links, and self
Prevention practitioners, links, and self
Strategy to find primary care physician for participants.
Not applicable
Prevention practitioners supported by primary care strategy engaging physicians and clinics near the clusters.
Primary outcome measures
Composite index, expressed as the ratio (multiplied by 100) of the number of eligible CDPS (chronic disease prevention and screening) actions at baseline (denominator) that were subsequently met at follow-up (numerator), measured at the patient level. (G*)
Ascertainment of outcomes
Abstraction from EMR and self-report responses at repeat self-administered survey by prevention practitioner
Self-report responses to survey administered by research assistant
For more information about the BETTER HEALTH: Durham study, please contact Dr. Lawrence Paszat at LawrencePaszat@sunnybrook.ca
Published results from the BETTER HEALTH: Durham study can be found here:
This project involved collaboration between the BETTER Program and the TAPESTRY (Teams Advancing Patient Experience: Strengthening Quality) Project. The goal of TAPESTRY is to promote optimal aging. Optimal aging within the TAPESTRY program means supporting people to move through life with good health in the best possible way: Being Alive Well.
The aim of this collaboration was to refine and integrate electronic versions of the BETTER Program tools (i.e. the BETTER App) into the TAPESTRY Application (or TAP-App) platform developed for use in the McMaster personal health record. Three primary care clinics, one in Alberta and two in Newfoundland & Labrador, will be asked pilot the e-tool enhanced BETTER approach and designate one or more personnel to undertake the role of Prevention Practitioner.
The Prevention Practitioner is a member of the team who receives training on the BETTER approach to chronic disease prevention and screening (CDPS), including shared decision-making and motivational interviewing. Using the BETTER App, and existing TAP-App tools as appropriate, the Prevention Practitioner worked directly with patients by inviting them to a special prevention visit at which an individualized “prevention prescription” was developed and patients were able to set their own CDPS goals. The Prevention Practitioner followed patients over time to assess their progress on their goals and their achievement/completion of the CDPS manoeuvers they were eligible to receive.
This project provided an opportunity to:
Determine how CDPS information should be best collected from patients through the BETTER App, and TAP-App tools as appropriate,
Understand
the feasibility and usability of the BETTER App and TAP App tools from
the perspectives of patients and primary care providers, and
Explore how the BETTER and TAP Apps and processes can help inform the care delivered to patients.
The desired long-term goals of the TAPESTRY-BETTER collaboration are to enhance patients’ care by:
Informing patients about their CDPS status through the use of the BETTER App and TAP App tools,
Enhancing
primary care providers/teams’ processes of care through the
personalization of the CDPS care delivered to patients, and
Increasing and streamlining the collaboration between patients and primary care.
For more information about the TAPESTRY project, please visit their website.
Through the BETTER Trial, we developed and tested a unique, comprehensive and integrated approach to chronic disease prevention and screening at the patient level.
To assess the adaptability, sustainability and effectiveness of the Prevention Practitioner intervention in other settings, including rural and remote settings, the BETTER approach was expanded into the Northwest Territories and Newfoundland & Labrador, and disseminated in Alberta, Ontario and Nova Scotia.
The BETTER 2 Program engaged patients, clinicians, researchers and policy-makers to develop an integrated, comprehensive, longitudinal and sustainable approach to chronic disease prevention and screening within the various settings. The BETTER 2 team also adapted and refined the BETTER tools, maneuvers, and training resources in order to increase feasibility and sustainability of the approach.
The specific aims of the BETTER 2 Program were:
To expand the BETTER approach into three new jurisdictions and
deepen the impact in the existing provinces by providing a framework,
tools and resources to do chronic disease prevention and screening.
To
further adapt, revise and tailor the BETTER individual patient-level
chronic disease prevention and screening intervention including the
survey, tools, maneuvers and resources to each setting including remote,
rural and disadvantaged populations (such as aboriginal populations and
populations with mental illness and substance abuse).
Evaluate
the adapted BETTER individual patient intervention including a
qualitative program evaluation of perceived effectiveness, facilitators
and barriers, benefits and disadvantages in varied settings including
remote, rural and disadvantaged populations.
Synthesize BETTER knowledge products for translation, dissemination and exchange.
To
develop a sustainable coalition and linkages between primary care
clinicians, researchers and policy-makers and evaluate the efforts of
the Coalition for sustained work on chronic disease prevention and
screening in primary care.
Each primary care setting wishing to implement the BETTER approach to chronic disease prevention and screening adapted the BETTER tools and approach to their setting and/or identified one or more personnel available to the practice to take on the role Prevention Practitioner. This individual:
Developed skills in chronic disease prevention and screening
Adapted the BETTER maneuvers and tools to their setting so that they are culturally relevant and sensitive
Identified resources to integrate into the practice
Developed a process within their setting for chronic disease prevention and screening
Identified which patients are ideal to target in their setting
Met with patients to develop individualized chronic disease prevention and screening prescriptions
More information about this implementation phase of the BETTER Program, can be found in our publications section.
For a downloadable version of the BETTER 2 Program Executive Summary, please click here.
The BETTER 2 Program Team (2012 – 2015)
Principal Investigators: Dr. Donna Manca and Dr. Eva Grunfeld Co-Investigators: Dr. Kris Aubrey-Bassler and Dr. Kami Kandola Dissemination Leads: Dr. Catherine Cervin, Dr. Emily Marshall, Dr. Nandini Natarajan, Dr. Sarah Newbery. Collaborators: P. Corcoran-Mooney, D. Gallant. Methodology Working Group: E. Grunfeld (Co-Chair), D. Manca (Co-Chair), K. Aubrey-Bassler, V. Faria, K. Kandola, P. Krueger, C. Meaney, R. Moineddin, C. Nykiforuk, N. Sopcak. Qualitative Methodology Working Group: N. Sopcak (Lead), C. Aguilar, L. Green, E. Grunfeld, P. Krueger, D. Manca, E. Marshall, C. Nykiforuk, M.A. O’Brien, G. Salvalaggio. Clinical Working Group: D. Campbell-Scherer (Chair), K. Aubrey-Bassler, J. Carroll, V. Faria, E. Grunfeld, J. Inman, K. Kandola, D. Klein, C. Korownyk, L. Lyall, D. Manca, J. Mercer, J. Neudorf, G. Salvalaggio, G. Stagg-Sturge, M. Wilson. Statistical Analysis: R. Moineddin, C. Meaney. Program Coordination: C. Fernandes, J. Baxter, R. Cullen, V. Faria. Research Assistant: M. Heatherington. Students/Trainees: Y. Khakhuda, M. Lukasewich.
The purpose of the BETTER Trial was to determine whether prevention and screening for cancer and other chronic diseases such as diabetes and heart disease could be improved in the family practice setting.
BETTER was a pragmatic cluster randomized controlled trial (RCT) predicated on the Ontario Ministry of Health and Long Term Care’s Chronic Disease Prevention and Management Framework.
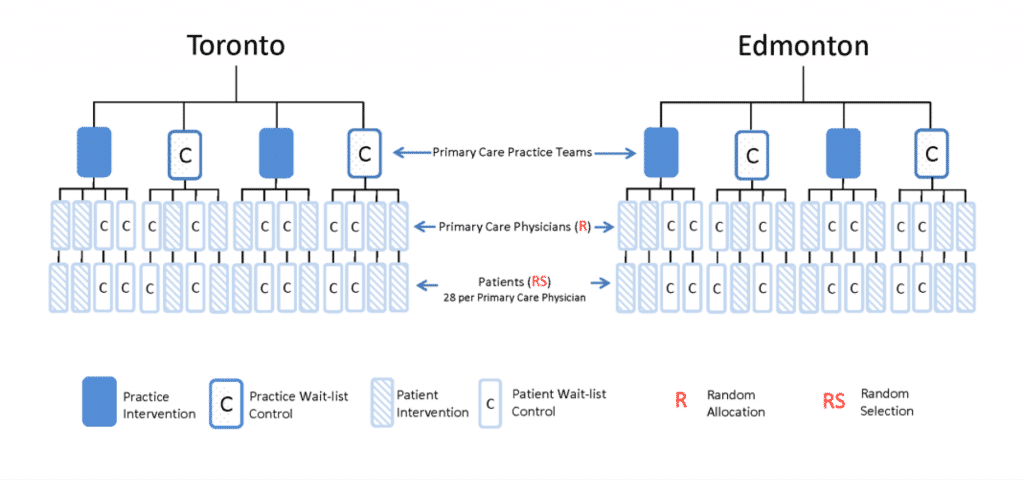
The setting for the BETTER Trial was eight, urban, Primary Care Team (PCT) practices in two Canadian jurisdictions (Toronto, Ontario and Edmonton, Alberta). PCTs are integrated primary care delivery models that include an inter-professional team. They work collaboratively to provide comprehensive, accessible, and coordinated primary healthcare to their rostered patients. The team typically comprises a combination of primary care physician (PCP), nurse practitioner, nurse, dietitian, pharmacist and other healthcare professional members.
Eight PCTs participated in BETTER, 4 in each jurisdiction, and 4 primary care physicians (PCPs) within each PCT participated as well, for a total of 32 PCPs (16 in each jurisdiction). Two PCTs in each jurisdiction were randomly allocated to the practice-level intervention arm. Within each PCT, two of the four participating Primary Care Physicians (PCPs) were randomly allocated to the patient-level intervention arm, for a total of 16 PCPs between both jurisdictions.
Therefore, the two-way factorial design produced:
Eight PCPs whose patients received the practice-level intervention only;
Eight PCPs whose patients received the patient-level intervention only;
Eight PCPs whose patients received both the practice-level and patient-level interventions;
Eight PCPs whose patients and practice continued to receive usual care.
The patient-level facilitation intervention involved 8 Prevention Practitioners (1 per PCT), who were healthcare professionals available within each PCT and chosen by the practice to undertake the role. The Prevention Practitioners received specialized training in the BETTER approach to evidence-based prevention and screening maneuvers and was responsible for meeting with patients one-on-one to assess their risk for chronic disease and helping them set chronic disease prevention and screening (CDPS) goals (i.e. the “Prevention Visit”). Through shared decision-making, the Prevention Practitioner and the patient developed a “Prevention Prescription” tailored specifically to that patient based on their medical and family history, and chronic disease risk. This personalized Prescription may have included referrals for screening procedures and/or referrals for lifestyle modification programs as appropriate.
The practice-level facilitation intervention involved 2 Practice Facilitators (1 per jurisdiction), who were individuals from outside the practice, trained in the BETTER approach to CDPS. Each Practice Facilitator was trained by the Centre for Effective Practice (CEP) and Quality Improvement and Innovation Partnership (QIIP) to work with representatives of each PCT to develop CDPS care paths for each maneuver used in BETTER. Each Practice Facilitator assessed the practices’ use of their electronic medical record (EMR) and prepared a “Prevention Prescription” aimed to better enable the EMR for CDPS (e.g. patient invitation letters, audit and feedback, decision support) and tailored to the needs of each PCT, with a focus on optimizing the use of information tools and resources available to the practice.
BETTER Results
Recruitment for BETTER started in August 2010 and ended in March 2011, resulting in the enrollment of 789 patients aged 40-65. Analysis shows a strong positive effect of the patient-level facilitation intervention and a minor effect of the practice-level facilitation intervention.
Several outputs were also generated as a result of the BETTER Trial:
Evidence-based care paths for each chronic disease prevention and screening maneuver, including tools and a toolkit tailored to the primary care setting;
The BETTER algorithm, which is a useful tool to inform clinicians on how to approach chronic disease prevention and screening; and
Patient education and motivational interviewing tools that aid clinicians in their assessment of each patient’s individual risks for chronic disease and the patient’s readiness to change.
More information about the BETTER cluster randomized controlled trial, can be found in our publications section.
The BETTER trial was made possible through a financial contribution from Health Canada, through the Canadian Partnership Against Cancer’s Coalitions Linking Action & Science for Prevention (CLASP) initiative, and from the Heart and Stroke Foundation of Canada.
The BETTER Trial Team (2009 – 2012)
Principal Investigators: Dr. Eva Grunfeld and Dr. Donna Manca Methodology Working Group: E. Grunfeld (Chair), D. Manca, R. Moineddin, K. Thorpe, M. Mamdani, P. Krueger. Clinical Working Group: D. Campbell-Scherer (Chair), R. Barrett, S. Bell, S. Bible, S. Buchman, J. Carroll, M. Dhaliwal, S. Dunn, M. Griever, E. Grunfeld, C. Harrison, L. Hosford, M. Kahan, D. Klein, C. Korownyk, K. Lang-Robertson, D. Manca, J. Meuser, V. Mozgala, J. Pencharz, L. Radmanovich, J. Rogers, G. Salvalaggio, L. Schaar, R. Stoller, D.L. Vesik, R. Wymer, M. Yan. Statistical Analysis: R. Moineddin, K. Thorpe, C. Meaney. Trial Coordination: Applied Health Research Centre, L. Patterson, C. Fernandes. Economic Analysis: J. Hoch, J. Beca. Research Assistants: T.K. Dallman, K. Kam, M. Leyland, P. Patel, D. Sanderson, C. Wright.
We can do BETTER – Building on Existing Tools to Improve Cancer and Chronic Disease Prevention and Screening in Primary Care Mainpro+ Workshop
The BETTER Program is currently accredited by The College of Family Physicians of Canada as a Maintenance of Proficiency (MainPro+) program. Participants can claim up to 3 MainPro+ credits for participating in a 3-hour workshop and completing a post-session self-reflective exercise, however, sessions can be tailored to accommodate different time constraints.
Additional information on MainPro accreditation can be found here.
Whenever possible, primary care professionals from diverse backgrounds, family medicine, nursing, pharmacy, etc. are encouraged to participate in the sessions as participants can learn from one another through sharing of differing perspectives and experiences.
Learning Objectives
Identify how to enhance the quality of care in your practice by integrating the best evidence for prevention and screening.
Identify how to incorporate prevention and health promotion in a clinical encounter in your practice.
Recognize how to engage patients and health professionals in shared decision-making to develop a plan of care (prevention prescription).
Identify how you can apply an intervention in your practice to improve prevention and screening.
Recognize how to work with others to assess, plan, provide, and integrate prevention and screening care for individual patients.
Identify how you could evaluate prevention and screening outcomes.
Session Description
The BETTER trial and subsequent studies have demonstrated that training a clinician to become a Prevention Practitioner, an individual within the primary care setting who develops specialized skills in cancer and chronic disease prevention and screening, significantly improved prevention and screening in patients 40-65 years of age as measured by a composite outcome. The BETTER approach: 1) is personalized to the patient and the practice; 2) addresses multiple conditions, including lifestyle factors; 3) is integrated with local, regional and national resources; and 4) is longitudinal, assessing patients over time. Through group discussions, participants will explore how they can adapt this novel, effective approach to their settings. The resources and tools developed to support this approach will be shared.
For more information about upcoming sessions or if you are interested in holding a BETTER MainPro+ session in your area, please contact us.